Update Latest
This commit is contained in:
143
Associate Degree/PSYG2500 Abnormal Psychology/01a.md
Normal file
143
Associate Degree/PSYG2500 Abnormal Psychology/01a.md
Normal file
@@ -0,0 +1,143 @@
|
||||
# 1.1 Introduction to Abnormal Psychology
|
||||
|
||||
### Course Objectives:
|
||||
|
||||
This course aims at providing students with a survey of
|
||||
behavioral disorders in terms of the biological,
|
||||
psychological, and sociocultural constellation of the
|
||||
person.
|
||||
While several orientations to the study of psychological
|
||||
disorders will be discussed, the primary emphasis will
|
||||
be put on the scientific study of these disorders from an
|
||||
empirical perspective
|
||||
|
||||
### Course Intended Learning Outcomes:
|
||||
|
||||
Describe and explain the symptomatology, etiology and
|
||||
therapy of various disorders introduced in the course
|
||||
using a biopsychosocial perspective;
|
||||
Apply their understanding of symptomatology and
|
||||
etiology and make a diagnosis based on presenting
|
||||
symptoms and suggest evidence-based treatments; and
|
||||
Explore and analyze the emotional, physical, and
|
||||
medical, implications of psychopathologies.
|
||||
Describe and explain the symptomatology, etiology and
|
||||
therapy of various disorders introduced in the course
|
||||
using a biopsychosocial perspective;
|
||||
Apply their understanding of symptomatology and
|
||||
etiology and make a diagnosis based on presenting
|
||||
symptoms and suggest evidence-based treatments; and
|
||||
Explore and analyze the emotional, physical, and
|
||||
medical, implications of psychopathologies.
|
||||
|
||||
## What Do We Mean By Abnormality?
|
||||
|
||||
### Indicators of Abnormality
|
||||
|
||||
- Subjective Distress
|
||||
- Maladaptiveness
|
||||
- Statistical Deviancy
|
||||
- Violation of the Standards of Society
|
||||
- Social Discomfort
|
||||
- Irrationality and Unpredictability
|
||||
- Dangerousness
|
||||
|
||||
### Mental Disorder
|
||||
|
||||
- Associated with distress or disability.
|
||||
- Biological, psychological, or developmental dysfunction in individual.
|
||||
- Clinically significant disturbance in behavior, emotional regulation,
|
||||
or cognitive function.
|
||||
|
||||
## Classification and Diagnosis
|
||||
|
||||
### Advantages of Classification Systems
|
||||
|
||||
- Provide nomenclature and common language
|
||||
- Allow information structuring
|
||||
- Facilitate research
|
||||
- Establish the range of problems to address
|
||||
|
||||
### Disadvantages of Classification
|
||||
|
||||
- Loss of individual’s information
|
||||
- Stigma and stereotyping associated with diagnosis
|
||||
- Self-concept impacted by diagnostic labeling
|
||||
|
||||
### Is there Any Way for US To Reduce Prejudicial Attitudes Toward People Who Are
|
||||
Mentally ill?
|
||||
|
||||
*Arthur and Colleagues (2010)*
|
||||
|
||||
- Negative reactions are widespread global phenomena
|
||||
- Understanding of neurobiological basis does not lessen
|
||||
stigma
|
||||
- Actual contact with individuals does lessen stigma
|
||||
|
||||
## Culture and Abnormality
|
||||
|
||||
- Presentation of disorders found worldwide
|
||||
- Certain forms of highly culture-specific psychopathology
|
||||
|
||||
## How Common Are Mental Disorders?
|
||||
|
||||
Significant question for many reasons:
|
||||
Planning, establishing, and funding mental health services for specific disorders;
|
||||
Providing clues to causes of mental disorders.
|
||||
|
||||
### Epidemiology
|
||||
|
||||
**Epidemiology:** Study of distribution of diseases, disorders, or health-related
|
||||
behaviors in a given population.
|
||||
|
||||
**Prevalence:** Number of active cases in population during any given period of
|
||||
time. Different types of prevalence estimates (point, 1-year, lifetime).
|
||||
|
||||
**Incidence:** Number of new cases in population over given period of time. Incidence figures are typically lower than prevalence figures
|
||||
|
||||
### Treatment
|
||||
|
||||
- Not all people receive treatment
|
||||
- Vast majority of treatment is done on outpatient basis
|
||||
- Inpatient hospitalization typically in psychiatric units
|
||||
|
||||
### Mental Health Professionals
|
||||
|
||||
#### Diagnosis and assessment involves participants who:
|
||||
|
||||
- Play differing roles in the process
|
||||
- Gather comprehensive evaluation patient data
|
||||
|
||||
#### Related Jobs including:
|
||||
|
||||
- Clinical Psychologist
|
||||
- Educational Psychologist
|
||||
- Counseling Psychologist
|
||||
- School Psychologist
|
||||
- Psychiatrist
|
||||
- Clinical Social Worker
|
||||
- Psychiatric Nurse
|
||||
- Occupational Therapist
|
||||
- Pastoral Counselor
|
||||
|
||||
## Research Approaches in Abnormal Psychology
|
||||
|
||||
### Benefits of Research
|
||||
• Learn about a disorder’s symptoms, prevalence,
|
||||
duration (acute, chronic), and accompanying problems
|
||||
• Understand etiology and nature of disorder
|
||||
• Discover how to provide the best patient care
|
||||
|
||||
## Sources of Information
|
||||
|
||||
**Case studies: **
|
||||
Specific individual observed and described in detail.
|
||||
Subject to bias of author of case study.
|
||||
|
||||
**Self-report data:**
|
||||
Participants asked to provide information about themselves.
|
||||
Interviews.
|
||||
|
||||
**Observational approaches:**
|
||||
Collecting information without asking participants directly for it.
|
||||
Outward behavior can be observed directly.
|
||||
201
Associate Degree/PSYG2500 Abnormal Psychology/01b.md
Normal file
201
Associate Degree/PSYG2500 Abnormal Psychology/01b.md
Normal file
@@ -0,0 +1,201 @@
|
||||
# 1.2 Historical and Contemporary Views of Abnormal Behavior
|
||||
|
||||
## Historical Views of Abnormal Behavior
|
||||
|
||||
### Demonology, Gods, and Magic
|
||||
|
||||
1. Abnormal behavior attributed to demonic possession
|
||||
1. Differentiated good vs. bad spirits based on the individual’s symptoms
|
||||
2. Religious significance of possession
|
||||
2. Primary treatment for demonic possession was exorcism
|
||||
a. Various techniques including magic, prayer, incantation,
|
||||
noisemaking, and use of horrible-tasting concoctions
|
||||
|
||||
### Hippocrates (460-377 B.C) Early Medical Concepts from Greek
|
||||
|
||||
- Proposing that mental disorders had natural
|
||||
causes
|
||||
- Categorizing disorders as mania, melancholia,
|
||||
or phrenitis
|
||||
- Associating dreams and personality
|
||||
|
||||
### Early Philosophical Conceptions of Consciousness
|
||||
|
||||
#### Plato (429-347 B.C.)
|
||||
|
||||
- Viewed psychological phenomena as responses of the
|
||||
whole organism
|
||||
- In The Republic, he emphasized individual differences and
|
||||
sociocultural influences
|
||||
- Discussed hospital care
|
||||
- Believed that mental disorders were in part divinely
|
||||
caused
|
||||
|
||||
#### Aristotle (384-322 B.C.)
|
||||
|
||||
- Wrote lasting description of consciousness
|
||||
- “Thinking” as directed would eliminate pain,
|
||||
attain pleasure
|
||||
|
||||
### Later Greek and Roman Thought
|
||||
|
||||
- **Egyptian:** proposed wide range of therapeutic measures like dieting, massage, hydrotherapy, gymnastics and education.
|
||||
- **Greek:** proposed disease based on flow of atoms through the pores in the body.
|
||||
Galen from Greek (130-200) provided anatomy of nervous system.
|
||||
- **Roman:** medicine focused on comfort.
|
||||
|
||||
### Early Views of Mental Disorders in China
|
||||
|
||||
- One of earliest foci on mental disorders (2674 B.C.)
|
||||
- Emphasis on natural causes
|
||||
- Chung Ching: “Hippocrates of China”
|
||||
- Experienced brief “Dark Ages” that blamed supernatural causes (late 200-900 A.D.)
|
||||
- Incorporation of ideas from Western psychiatry in last 50 years
|
||||
|
||||
### Views of Abnormality During the Middle Ages
|
||||
|
||||
- **Middle East:** had scientific approach.
|
||||
- **Europe:** was plagued with mass madness.
|
||||
- Relating the mental illness with witchcraft, and treatment included exorcism
|
||||
|
||||
## Toward Humanitarian Approaches
|
||||
|
||||
### The Resurgence of Scientific Questioning in Europe
|
||||
|
||||
**Renaissance:**
|
||||
|
||||
- Led to resurgence of scientific questioning in
|
||||
Europe
|
||||
- Part of humanism movement
|
||||
|
||||
### The Establishment of Early Asylums
|
||||
|
||||
- First established in Sixteenth Century
|
||||
- “Madhouses”“Bedlam” storage places for the insane
|
||||
- Found throughout Europe; parts of U.S.
|
||||
- Aggressive treatment to restore “physical balance in body and brain”
|
||||
|
||||
### Humanitarian Reform
|
||||
|
||||
- France:
|
||||
- Philippe Pinel (1745-1826)
|
||||
- unchained patients, placed them in sunny rooms and treated them with exercise and kindness
|
||||
- England:
|
||||
- William Tuke, Quakers (1732-1822)
|
||||
- established the York Retreat, a country house for the mentally ill. He treated with kindness and acceptance
|
||||
- America:
|
||||
- Benjamin Rush (1745-1813): emphasized spiritual and moral development
|
||||
- Benjamin Franklin (1706-1790): proposed using electricity to treat melancholia
|
||||
- Dorothy Dix (1802-1887): suitable hospitals were built
|
||||
|
||||
|
||||
#### The military’s role in mental health treatment:
|
||||
|
||||
- American Civil War (1861-1865)
|
||||
- First mental health facility opened
|
||||
- Germany (1870-1914)
|
||||
- Developed program of military psychiatry following FrancoPrussian War
|
||||
- Contributed to field of abnormal psychology
|
||||
|
||||
### Nineteenth-Century Views of the Causes and Treatment of Mental Disorders
|
||||
|
||||
**Alienists (psychiatrists):**
|
||||
|
||||
- Gained control of asylums
|
||||
- Emotional problems (“shattered nerves”) were caused by the expenditure of energy or by the depletion of bodily energies as a result of excesses in living
|
||||
|
||||
### Changing Attitudes Toward Mental Health in the Early Twentieth Century
|
||||
|
||||
**Clifford Beers (1876-1943):**
|
||||
|
||||
- Described own mental collapse in A Mind That Found Itself in 1908
|
||||
- Straitjacket was still widely used
|
||||
- Began campaign for reform
|
||||
|
||||
### Mental Hospital Care in the Twentieth Century
|
||||
|
||||
- 1940
|
||||
- Most mental hospitals inhumane and ineffective
|
||||
- 1946
|
||||
- Mary Jane Ward published The Snake Pit
|
||||
- National Institutes of Mental Health
|
||||
- Hill–Burton Act (funded community mental health hospitals)
|
||||
- 1963
|
||||
- Community Health Services Act (develop outpatient psychiatric clinics, community consultations, and rehab programs)
|
||||
|
||||
|
||||
#### Deinstitutionalization Movement
|
||||
|
||||
- Large numbers of mental hospital closures and shift to community-based residences
|
||||
- Global movement: Asia, Europe, U.S.
|
||||
- Considered more humane and cost effective
|
||||
- Created problems for both patients and society as a whole
|
||||
|
||||
|
||||
## The Emergence of Contemporary Views of Abnormal Behavior
|
||||
|
||||
### The Emergence of Contemporary Views of Abnormal Behavior
|
||||
|
||||
**Recent changes:**
|
||||
|
||||
1. Biological discoveries
|
||||
2. Development of mental disorders classification
|
||||
system
|
||||
3. Emergence of psychological causation views
|
||||
4. Experimental psychological research developments
|
||||
|
||||
### Biological Discoveries
|
||||
|
||||
1. Biological and anatomical factors recognized as underlying both physical and mental disorders
|
||||
2. Cure for general paresis (syphilis of the brain)
|
||||
- Raised hopes that organic bases would be found for many other mental disorders
|
||||
3. Mental disorders an illness based on brain pathology
|
||||
- Downside: removal of body parts, lobotomies
|
||||
|
||||
### The Development of a Classification System
|
||||
|
||||
**Kraepelin:**
|
||||
|
||||
- Compendium der Psychiatrie (1883): forerunner to DSM
|
||||
- Specific types of mental disorders identified
|
||||
|
||||
### Emergence of psychological causation views
|
||||
|
||||
#### Mesmerism:
|
||||
|
||||
- Diseases treated by “animal magnetism”
|
||||
- Source of heated discussion in early nineteenth century
|
||||
|
||||
#### Nancy School
|
||||
- Hypnotism and hysteria are related and due to suggestion
|
||||
- Hysteria, a form of self-hypnosis, could be caused and removed by hypnosis
|
||||
|
||||
**Nancy School–Charcot debate**
|
||||
|
||||
- Are mental disorders caused by biological or psychological factors?
|
||||
|
||||
#### Sigmund Freud (1856–1939)
|
||||
|
||||
- First major steps toward understanding psychological factors in
|
||||
mental disorders
|
||||
- Psychoanalytic perspective:
|
||||
- Catharsis (repressed emotions.)
|
||||
- The unconscious
|
||||
- Free association
|
||||
- Dream analysis
|
||||
- Emphasizes inner dynamics of unconscious motives
|
||||
|
||||
### Experimental psychological research developments
|
||||
- **Wilhelm Wundt:** First experimental psychological laboratory
|
||||
- **J. McKeen Cattell:** Wundt’s methods to U.S.
|
||||
- **Lightner Witmer:** First American psychological clinic
|
||||
|
||||
#### Behavioral perspective:
|
||||
|
||||
Role of learning in humanbehavior.
|
||||
|
||||
- Classical Conditioning
|
||||
- Neutral stimulus repeatedly paired with unconditioned stimulus; naturally elicits an unconditioned behavior
|
||||
- Ivan Pavlov, John B. Watson
|
||||
- Operant Conditioning
|
||||
- E. L. Thorndike, B. F. Skinner
|
||||
229
Associate Degree/PSYG2500 Abnormal Psychology/02.md
Normal file
229
Associate Degree/PSYG2500 Abnormal Psychology/02.md
Normal file
@@ -0,0 +1,229 @@
|
||||
# 2. Causes of Abnormal Behavior
|
||||
|
||||
## Risk Factors and Causes of Abnormal Behavior
|
||||
|
||||
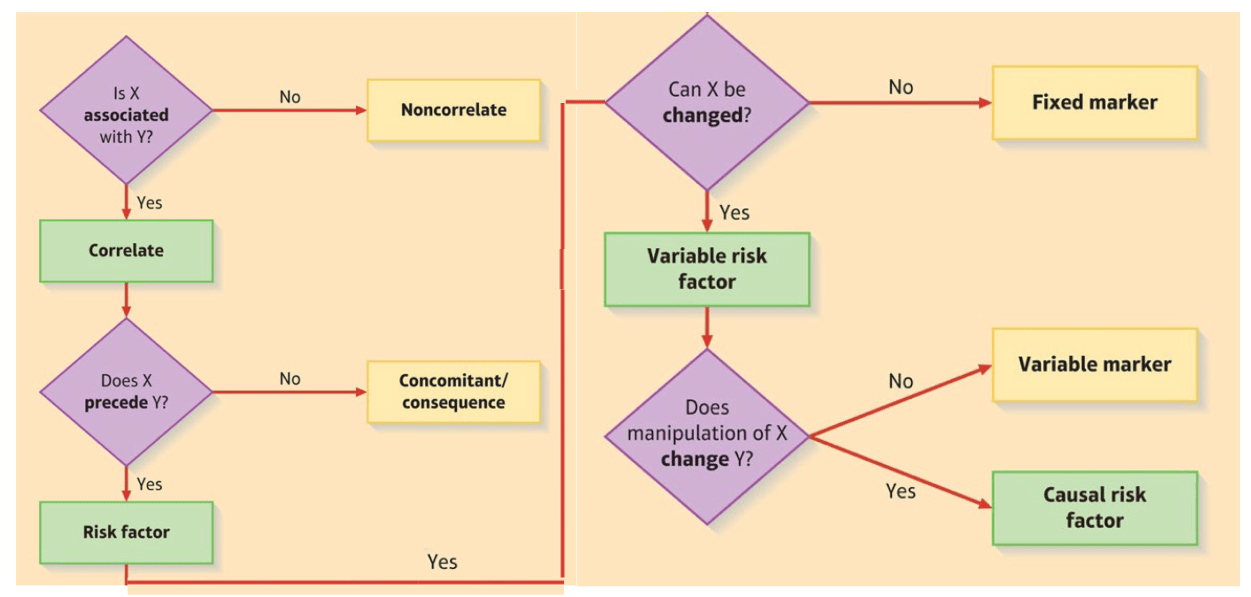
- A **necessary cause** (X) is a condition that must exist for a disorder (Y) to occur.
|
||||
- A **sufficient cause** of a disorder is a condition that guarantees the occurrence of a disorder.
|
||||
- A **contributory cause** is one that increases the probability of a disorder developing but is neither necessary nor sufficient for the disorder to occur.
|
||||
|
||||
### Causes of Abnormal Behavior
|
||||
|
||||
- **Distal risk factors** are causal factors occurring relatively early in life that may not show their effects for many years.
|
||||
- **Proximal (immediate) risk factors** are factors that operate shortly before the occurrence of the symptoms of a disorder.
|
||||
|
||||
|
||||
|
||||
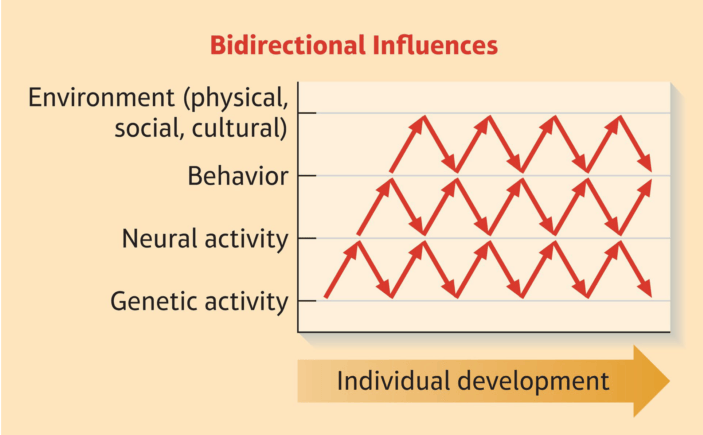
### Feedback and Bidirectionality in Abnormal Behavior
|
||||
|
||||
In the study of abnormal psychology, it can be challenging to determine with certainty which conditions are causes and which are effects due to the complex and bidirectional nature of mental health disorders.
|
||||
|
||||
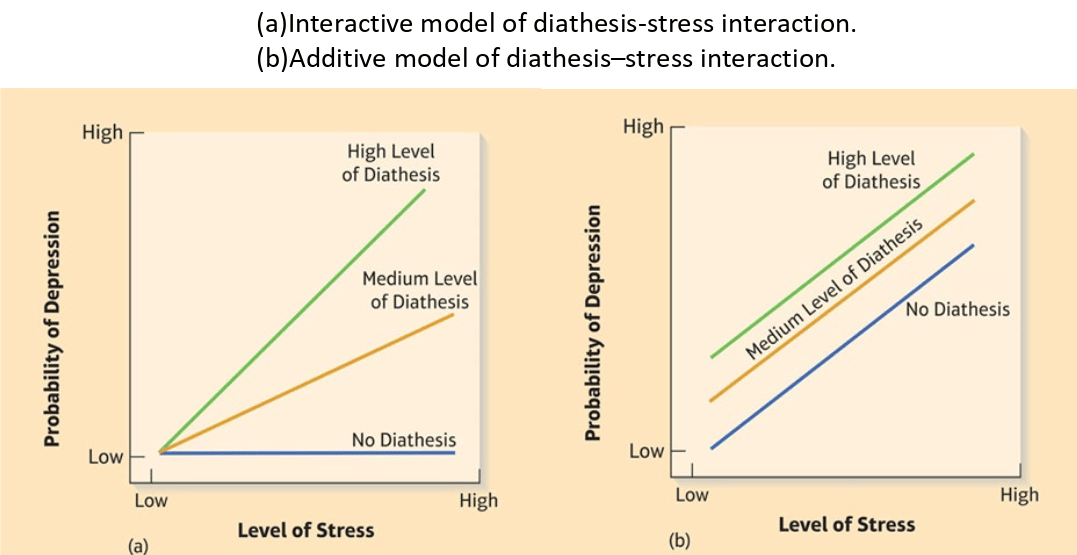
### Diathesis-Stress Models
|
||||
|
||||
Combination of diathesis and stress to cause disorder.
|
||||
|
||||
- Diathesis: Relatively distal necessary or contributory cause that is not sufficient to cause disorder
|
||||
- Stress: Response of individual to taxing demands.
|
||||
|
||||
|
||||
|
||||
### Protective factors
|
||||
|
||||
Stronger Resilience with:
|
||||
|
||||
- Healthy Family environment
|
||||
- Exposure to stressful experiences that are dealt with successfully
|
||||
- Emotional intelligence
|
||||
|
||||
## Perspectives to Understand the Causes of Abnormal Behavior
|
||||
|
||||
### The Biological Perspective
|
||||
|
||||
Four categories of biological factors relevant to maladaptive behavior.
|
||||
|
||||
#### Genetic vulnerabilities
|
||||
|
||||
Heredity is important predisposing contributory cause for number of disorders.
|
||||
|
||||
##### The Relationship of Genotypes to Phenotypes
|
||||
|
||||
**Genotype:** Total genetic endowment.
|
||||
|
||||
**Phenotype:** Observed structural and functional characteristics.
|
||||
|
||||
##### Methods for Studying Genetic Influences
|
||||
|
||||
**Traditional methods:**
|
||||
|
||||
- Family history method
|
||||
- Twin method
|
||||
- Adoption method
|
||||
|
||||
**More recent methods:**
|
||||
|
||||
- Linkage analysis
|
||||
- Association studies
|
||||
|
||||
#### Brain dysfunction and neural plasticity
|
||||
|
||||
Subtle deficiencies of brain function are rarely implicated in mental disorders.
|
||||
|
||||
Genetic programs for brain development are not as rigid and deterministic as was once believed.
|
||||
|
||||
The Developmental Systems Approach
|
||||
|
||||
|
||||
|
||||
#### Neuro-transmitter & hormonal abnormalities in brain and CNS
|
||||
|
||||
**Neurotransmitter imbalances:**
|
||||
|
||||
- Can result in abnormal behavior
|
||||
- Created in various ways: overproduction, deactivation, abnormally
|
||||
sensitive or insensitive
|
||||
|
||||
**5 Most studied neurotransmitter:**
|
||||
|
||||
- Norepinephrine
|
||||
- Dopamine
|
||||
- Serotonin
|
||||
- Glutamate
|
||||
- Gamma aminobutyric acid (GABA)
|
||||
|
||||
**Hormonal Imbalances**
|
||||
|
||||
Hypothalamic-pituitary-adrenal (HPA) axis:
|
||||
|
||||
- Messages (CRH) travel from the hypothalamus to the pituitary
|
||||
- Pituitary releases ACTH, which stimulates cortical part of the adrenal gland, produces epinephrine (adrenaline) and cortisol
|
||||
- Cortisol provides negative feedback to hypothalamus and pituitary to decrease their release of CRH and ACTH, which in turn reduces the release of adrenaline and cortisol
|
||||
|
||||
#### Temperament
|
||||
|
||||
**Temperament:**
|
||||
|
||||
Child’s reactivity and characteristic ways of self-regulation.
|
||||
Early temperament is basis from which personality develops.
|
||||
|
||||
**Five Dimensions of Temperament:**
|
||||
|
||||
- Fearfulness
|
||||
- Irritability and frustration
|
||||
- Positive affect
|
||||
- Activity level
|
||||
- Attentional persistence and effortful control
|
||||
|
||||
### The Psychological Perspective
|
||||
|
||||
#### Psychodynamic
|
||||
|
||||
**Freud** theorized that a person’s behavior results from interaction of:
|
||||
|
||||
- Id (pleasure principle)
|
||||
- Ego (reality principle)
|
||||
- Superego (executive branch)
|
||||
|
||||
**Newer Psychodynamic Perspectives:**
|
||||
|
||||
- Ego psychology
|
||||
- Attachment theory
|
||||
- Object-relations theory
|
||||
- Interpersonal perspective
|
||||
|
||||
#### Behavioral
|
||||
|
||||
- Classical Conditioning
|
||||
- Operant Conditioning
|
||||
- Generalization and Discrimination
|
||||
- Observational Learning
|
||||
|
||||
#### Cognitive-Behavioral
|
||||
|
||||
- **Schema:** Underlying representation of knowledge that guides current processing of information
|
||||
- **Attributions:** Process of assigning causes to things that happen
|
||||
- **Attributional style:** Characteristic way in which individual may tend to assign causes to bad or good events
|
||||
|
||||
**Cognitive Therapy:**
|
||||
|
||||
- The way we interpret events and experiences determines our emotional reactions to them.
|
||||
- Clinicians use a variety of techniques designed to alter a client’s negative cognitive biases.
|
||||
|
||||
### The Social Perspective
|
||||
|
||||
Factors with detrimental effects on a child’s socioemotional development.
|
||||
|
||||
#### Early deprivation or trauma
|
||||
|
||||
- Depriving essential resources
|
||||
- Institutionalization
|
||||
- Neglect and abuse at home
|
||||
- Separation from parents
|
||||
|
||||
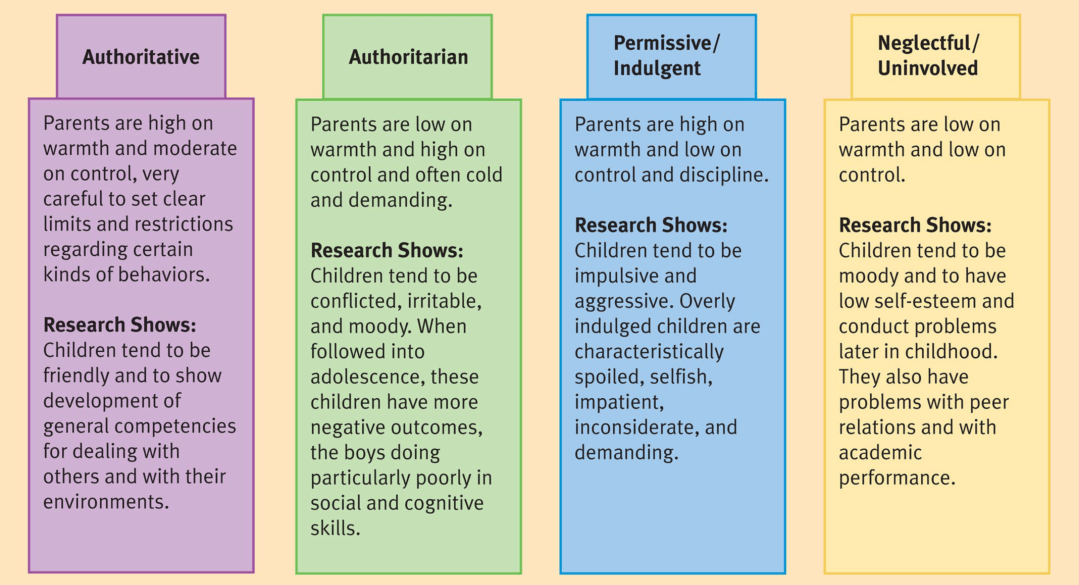
#### Problems in parenting style
|
||||
|
||||
A parent–child relationship is always bidirectional:
|
||||
Parents who have various forms of psychopathology tend to have one or more children at heightened risk for a wide range of developmental difficulties.
|
||||
|
||||
|
||||
|
||||
#### Marital discord & divorce
|
||||
|
||||
**Long-standing marital discord:**
|
||||
|
||||
- Aggressive behavior
|
||||
- Poor quality relationships
|
||||
|
||||
**Divorce:**
|
||||
|
||||
- Insecurity, rejection
|
||||
- Delinquency
|
||||
- Lower educational attainment
|
||||
|
||||
#### Low Socioeconomic Status and Unemployment
|
||||
|
||||
In our society, the lower the socioeconomic class, the higher the incidence of mental and physical disorders.
|
||||
|
||||
- Children and adolescents from lower socioeconomic status (SES) families tend to have more psychological problems.
|
||||
- Studies have repeatedly found unemployment to be associated with enhanced vulnerability to psychopathology.
|
||||
|
||||
#### Maladaptive peer relation-ships
|
||||
|
||||
- Peer exclusion or abuse
|
||||
- Proactive and reactive aggression in bullying
|
||||
- Cyberbullying
|
||||
|
||||
#### Prejudice and Discrimination in Race, Gender, and Ethnicity
|
||||
|
||||
Increased prevalence of certain mental disorders may be related to:
|
||||
|
||||
- Prejudice against minority groups and women
|
||||
- Perceived discrimination and self-esteem
|
||||
|
||||
### The Cultural Perspective
|
||||
|
||||
**Cultural context of behavior:**
|
||||
|
||||
- Universal and Culture-Specific Symptoms of Disorders
|
||||
- Culture: Over-and Undercontrolled Behavior
|
||||
|
||||
#### Universal and Culture-Specific Symptoms of Disorders
|
||||
|
||||
**Universality of some disorders:**
|
||||
|
||||
- Certain psychological symptoms are consistently found among similarly diagnosed clinical groups
|
||||
|
||||
**Sociocultural factors:**
|
||||
|
||||
- Which disorders develop
|
||||
- Prevalence, course
|
||||
|
||||
#### Culture: Over- and Undercontrolled Problem
|
||||
|
||||
**Undercontrolled problem:**
|
||||
|
||||
- Agression, disobedience, disrespect
|
||||
- Exhibited by American
|
||||
|
||||
**Overcontrolled problem:**
|
||||
|
||||
- Shyness, anxiety, depression
|
||||
- Exhibited by Thai
|
||||
180
Associate Degree/PSYG2500 Abnormal Psychology/03.md
Normal file
180
Associate Degree/PSYG2500 Abnormal Psychology/03.md
Normal file
@@ -0,0 +1,180 @@
|
||||
# 3. Assessment of Mental Health Problems
|
||||
|
||||
## Introduction to Basic Elements in Assessment
|
||||
|
||||
Interaction of **Importance of trust and rapport** and **Impact on assessment** process.
|
||||
|
||||
### Identification of presenting problem
|
||||
|
||||
- Situational or pervasive?
|
||||
- Duration?
|
||||
- Prior attempts to help or treat?
|
||||
- Self-defeating or resourceful?
|
||||
- How does problem impact social roles?
|
||||
- Does problem match any DSM-5 disorder criteria?
|
||||
|
||||
### Advantage of classification of presenting problem
|
||||
|
||||
- Treatment planning
|
||||
- Knowledge of range of diagnostic problems
|
||||
- Insurance payment
|
||||
|
||||
### Good assessment includes
|
||||
|
||||
- social history noting:
|
||||
- Personality factors
|
||||
- Social context
|
||||
- various professional orientations:
|
||||
- May determine assessment techniques
|
||||
- Does not limit clinician to one type of assessment
|
||||
|
||||
### Dynamic formulation
|
||||
|
||||
Describes the current situation but also includes hypotheses about what is driving the person to behave in maladaptive ways.
|
||||
|
||||
- Hypotheses about future behavior are derived.
|
||||
- Decisions about treatment are made collaboratively with the consent and approval of the individual.
|
||||
- Assessment may involve the coordinated use of physical, psychological, and environmental procedures.
|
||||
|
||||
### Psychological Assessments are
|
||||
|
||||
- Reliable
|
||||
- Valid
|
||||
- Standardized
|
||||
|
||||
## Assessment of the Physical Conditions
|
||||
|
||||
### General physical examination
|
||||
|
||||
Many psychological problems have physical components either as
|
||||
|
||||
- Causal factors
|
||||
- Symptom patterns
|
||||
|
||||
### Neurological examination
|
||||
|
||||
- **EEG:** graphical record of brain’s electrical activity
|
||||
- **CAT scan & MRI:** images of brain structures that may be damaged or diseased
|
||||
- **PET scan:** metabolic activity of specific compounds
|
||||
- **fMRI:** mapping psychological activity to specific regions in the brain
|
||||
|
||||
### Neuro-psychological examination
|
||||
|
||||
- Involves use of expanding array of testing devices
|
||||
- Measures cognitive, perceptual, and motor performance
|
||||
- Provides clues to extent and location of brain damage
|
||||
|
||||
**Halstead-Reitan Neuropsychological Battery (HRNB) (10 tests in total):**
|
||||
|
||||
- **Halstead Category Test:** Learn & remember
|
||||
- **Tactual Performance Test**: Motor function, response, tactile & kinesthetic cues
|
||||
- **Rhythm Test:** Attention, sustained concentration
|
||||
- **Speech Sounds Perception Test:** Identify spoken words
|
||||
- **Finger Oscillation Task:** Speed
|
||||
|
||||
## Psychosocial Assessment
|
||||
|
||||
### Assessment Interviews
|
||||
|
||||
- Face-to-face interaction
|
||||
- Structured interviews
|
||||
- Unstructured interviews
|
||||
|
||||
### Clinical Observation of Behavior
|
||||
|
||||
- Clinical observation in natural environments
|
||||
- Clinical observations in therapeutic or medical settings
|
||||
- Self-monitoring
|
||||
|
||||
### Psychological Tests
|
||||
|
||||
#### Intelligence tests
|
||||
|
||||
- WISC-IV(children); WAISIV (adults)
|
||||
- Stanford-Binet
|
||||
|
||||
#### Personality tests
|
||||
|
||||
##### Projective personality tests
|
||||
|
||||
- Unstructured stimuli are presented
|
||||
- Meaning or structure projected onto stimuli
|
||||
- Projections reveal hidden motives
|
||||
|
||||
**Projective personality tests examples:**
|
||||
|
||||
- Rorschach Inkblot Test
|
||||
- Thematic Apperception Test (TAT)
|
||||
- Sentence Completion Test
|
||||
|
||||
##### Objective personality tests
|
||||
|
||||
Examples: NEO-PI, MMPI-2
|
||||
|
||||
Objective personality tests offer several advantages, such as standardization, efficiency, and ease of administration, but also have limitations, including limited depth, potential response distortion, and cultural bias.
|
||||
|
||||
## The Integration of Assessment Data
|
||||
|
||||
- Developing integrated, coherent working model
|
||||
- Utilizing individual or team approach
|
||||
- Identifying definitive picture vs. discrepancie
|
||||
|
||||
### Ethical Issues in Assessment
|
||||
|
||||
- Potential cultural bias
|
||||
- Theoretical orientation of clinician
|
||||
- Underemphasis on external situation
|
||||
- Insufficient validation
|
||||
- Inaccurate data or premature evaluation
|
||||
|
||||
## Classifying Abnormal Behavior
|
||||
|
||||
- Classification involves attempts to delineate meaningful sub-varieties of maladaptive behavior.
|
||||
- Classification makes it possible to communicate about particular clusters of abnormal behavior in agreed-on and relatively precise ways.
|
||||
- Classification of some kind is a necessary first step toward introducing order into our discussion of the nature, causes, and treatment of such behavior.
|
||||
- Classification enables the clarification of insurance issues.
|
||||
|
||||
### Differing Models of Classification
|
||||
|
||||
Three basic approaches include:
|
||||
|
||||
- Categorical approach:
|
||||
a patient is healthy or disordered, but there is no overlap
|
||||
- Dimensional approach:
|
||||
the patient may fall along a range from superior functioning
|
||||
to absolutely impaired functioning
|
||||
- Prototypal approach:
|
||||
a conceptual entity depicts an idealized combination of
|
||||
characteristics, some of which the patient may not have
|
||||
|
||||
### Formal Diagnostic Classification of Mental Disorders
|
||||
|
||||
- Diagnostic and Statistical Manual of Mental Disorders (DSM-5)
|
||||
- International Classification of Disease (ICD-10)
|
||||
|
||||
#### Definition criteria based on:
|
||||
|
||||
- Symptoms (subjective)
|
||||
- Signs (objective)
|
||||
|
||||
#### The DSM-5
|
||||
|
||||
- More comprehensive and more subtypes of disorders
|
||||
- Allows for gender related differences in diagnosis
|
||||
- Provides structured interview regarding cultural influences
|
||||
|
||||
#### Problem of diagnostic labeling
|
||||
|
||||
- Allows label capturing more than a behavioral pattern
|
||||
- Creates assumptions among clinicians
|
||||
- Creates social identity (stigma)
|
||||
|
||||
#### Diagnostic Interviews
|
||||
|
||||
- Unstructured:
|
||||
- Freewheeling
|
||||
- Clinician can follow leads
|
||||
- Clinical picture may vary, based on interviewer
|
||||
- Structured
|
||||
- Controlled
|
||||
- Determine if symptoms fit diagnostic criteria
|
||||
234
Associate Degree/PSYG2500 Abnormal Psychology/04.md
Normal file
234
Associate Degree/PSYG2500 Abnormal Psychology/04.md
Normal file
@@ -0,0 +1,234 @@
|
||||
# 4. Stress
|
||||
|
||||
## What Is Stress?
|
||||
|
||||
- External demands placed on an organism
|
||||
- Organism’s internal biological and psychological responses to such demands
|
||||
|
||||
### Behavioral Medicine
|
||||
|
||||
Concerned with psychological factors that may predispose an individual to medical problems: Health psychology
|
||||
The effects of stress and other psychological factors in the development and maintenance of physical problems
|
||||
|
||||
### Stress and *DSM*
|
||||
|
||||
- Significant component of multiple DSM diagnostic categories
|
||||
- DSM-5: Trauma- and stressor-related disorders
|
||||
|
||||
### Factors Predisposing a Person to Stress
|
||||
|
||||
- Experience of crisis
|
||||
- Life changes
|
||||
- Individual perception of stressor
|
||||
- Individual stress tolerance
|
||||
- Lack of external resources and social supports
|
||||
|
||||
### Characteristics of Stressors
|
||||
|
||||
Life changes, Crises, and Perception of benefits.
|
||||
|
||||
- Severity
|
||||
- Chronicity
|
||||
- Timing
|
||||
- Degree of impact
|
||||
- Level of expectation
|
||||
- Controllability
|
||||
|
||||
Measuring Life Stress
|
||||
|
||||
- Social Readjustment Rating Scale
|
||||
- Self-report checklist
|
||||
- Limited
|
||||
- Life Events and Difficulties Schedule
|
||||
- Interview-based
|
||||
- Rates chronic and acute stress
|
||||
|
||||
### Resilience
|
||||
|
||||
Factors linked to resilience:
|
||||
|
||||
- Male gender
|
||||
- Older age
|
||||
- Higher Eeducation
|
||||
- Economic resources
|
||||
- Positive thinking
|
||||
- Self confidence
|
||||
|
||||
## Stress and Physical Health
|
||||
|
||||
#### Allostatic load
|
||||
|
||||
Biological cost of adapting to stress.
|
||||
|
||||
- High load = more stress
|
||||
- Everyday forms of stress can also elevate risk for coronary heart disease and death
|
||||
- Mental stress raises blood pressure, migraine, and elevates epinephrine levels
|
||||
|
||||
#### The Stress Response
|
||||
|
||||
Two of body’s systems respond when stressor is perceived:
|
||||
|
||||
- **Sympathetic-adrenomedullary (SAM) system:** mobilize resources and enable the body to metabolize glucose more rapidly.
|
||||
- **Hypothalamus-pituitary-adrenal (HPA) system:** produce cortisol to enable the the body for fight or flight and promote escape behavior
|
||||
|
||||
### Stress and Immune System Functioning
|
||||
|
||||
#### The Mind-Body Connection
|
||||
|
||||
Stress may cause overall vulnerability to disease.
|
||||
|
||||
#### Understanding the Immune System
|
||||
|
||||
- Protects body from such things as viruses and bacteria
|
||||
- Provides leukocytes: front lines of defense
|
||||
- Communicates with brain via cytokines
|
||||
|
||||
#### Stress and Immune System Functioning
|
||||
|
||||
Stress is linked to immune system suppression
|
||||
- Short-term stress compromises immune system
|
||||
- Long-term stress associated with global immunosuppression
|
||||
|
||||
#### Chronic Stress and Inflammation
|
||||
|
||||
1. Long term stress
|
||||
2. Body cannot turn off cytokine production
|
||||
3. Chronic inflammation
|
||||
|
||||
Stress and Premature Aging
|
||||
|
||||
1. Stress
|
||||
2. Shortens telomere length
|
||||
3. Shorter telomeres affect cell function, increase disease risk
|
||||
|
||||
### Emotions and Health:
|
||||
|
||||
#### Personality Types
|
||||
|
||||
The Type A behavior pattern:
|
||||
|
||||
- Excessive competitive drive
|
||||
- Extreme commitment to work
|
||||
- Impatience and time urgency
|
||||
- Hostility
|
||||
|
||||
Type D Questionnaire:
|
||||
tendency to experience negative emotions and also to feel insecure and anxious
|
||||
|
||||
|
||||
|
||||
#### Emotion
|
||||
|
||||
- Depression: Associated with disrupted immune function beyond stressors that precipitated depressed mood
|
||||
- Anxiety
|
||||
- Phobic anxiety is linked to increased risk for sudden cardiac death
|
||||
- Social isolation and lack of social support
|
||||
- Lonely people at increased risk of developing heart disease
|
||||
- Positive emotions
|
||||
- Forgiveness may lower stress levels
|
||||
- Emotion regulation
|
||||
- Psychological well-being
|
||||
- Physical health
|
||||
|
||||
### Treatments of Stress-Related Physical Disorders
|
||||
|
||||
#### Biological Interventions
|
||||
|
||||
- Surgical procedures (handling problems for e.g. CHD)
|
||||
- Lipid-lowering medications: reduce anxiety
|
||||
- Aspirin: reduce pain
|
||||
- Antidepressant medications
|
||||
|
||||
#### Psychological Interventions
|
||||
|
||||
- Emotional disclosure
|
||||
- Biofeedback
|
||||
- Relaxation and meditation
|
||||
- Cognitive-behavior therapy
|
||||
|
||||
## Stress and Mental Health:
|
||||
|
||||
### Adjustment disorder
|
||||
|
||||

|
||||
|
||||
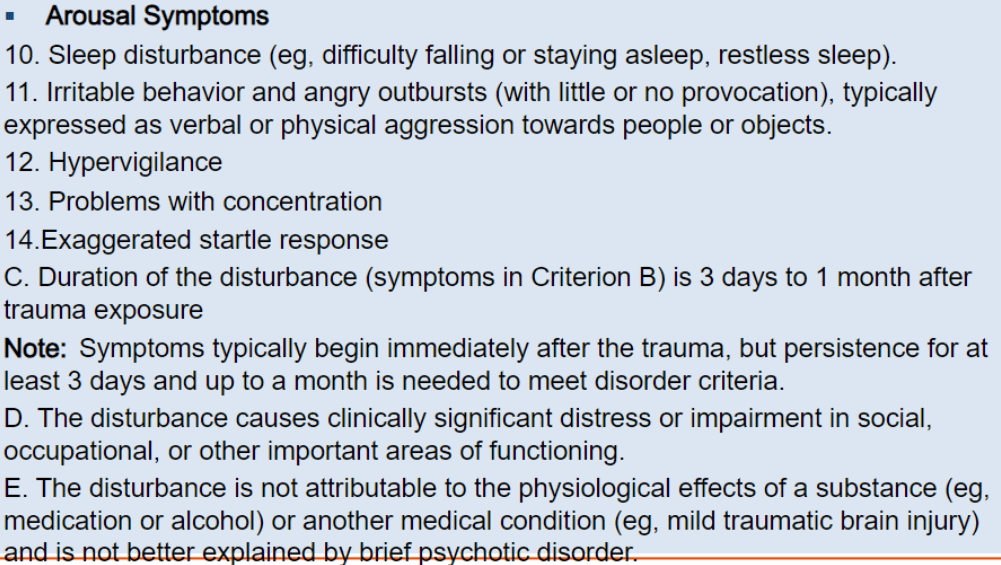
### Acute Stress Disorder
|
||||
|
||||
|
||||
|
||||
|
||||
|
||||
|
||||
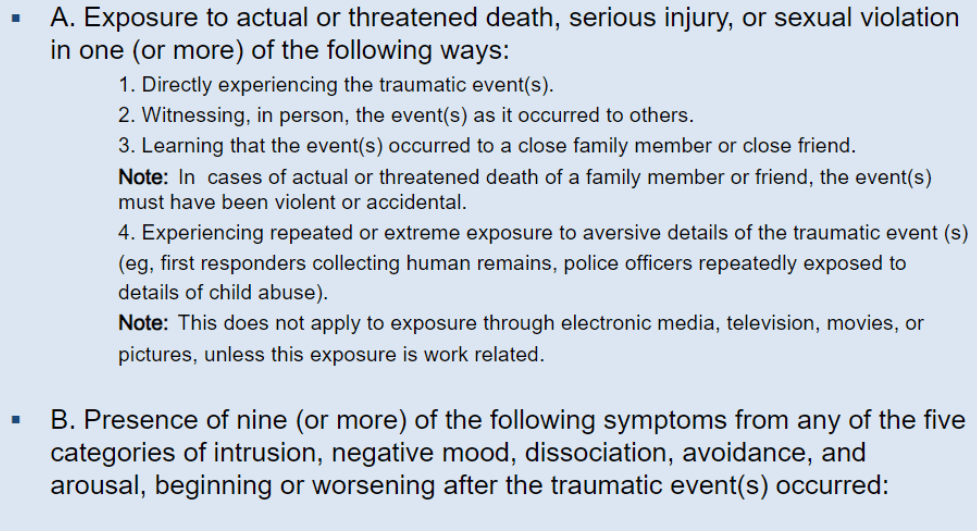
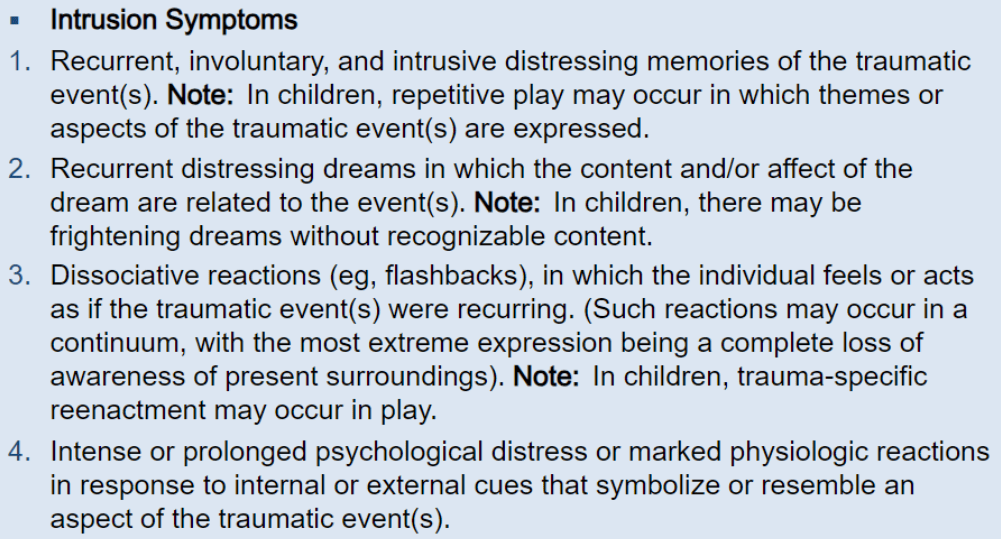
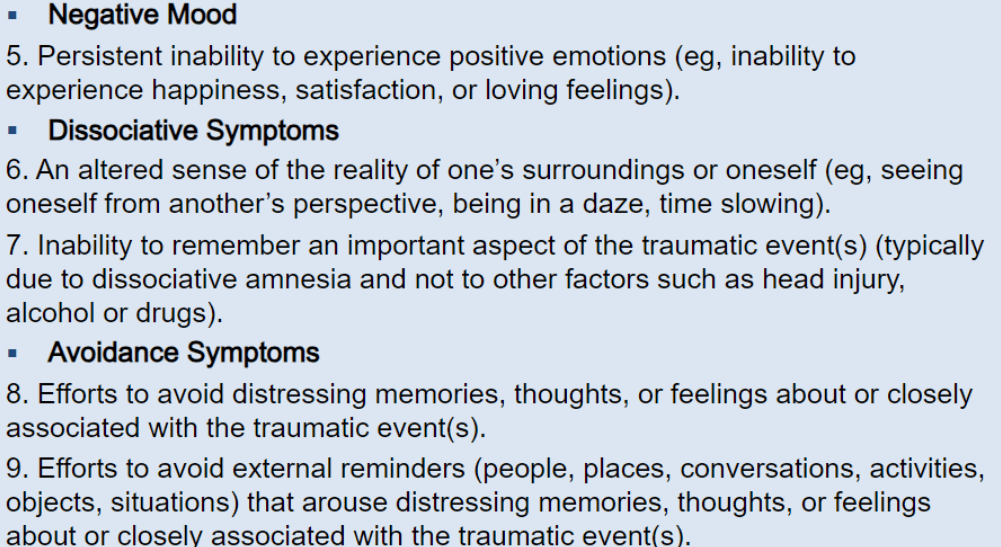
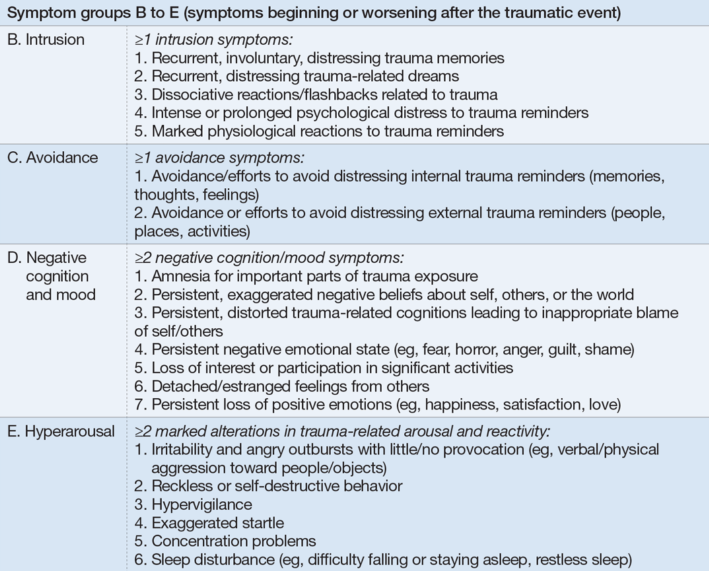
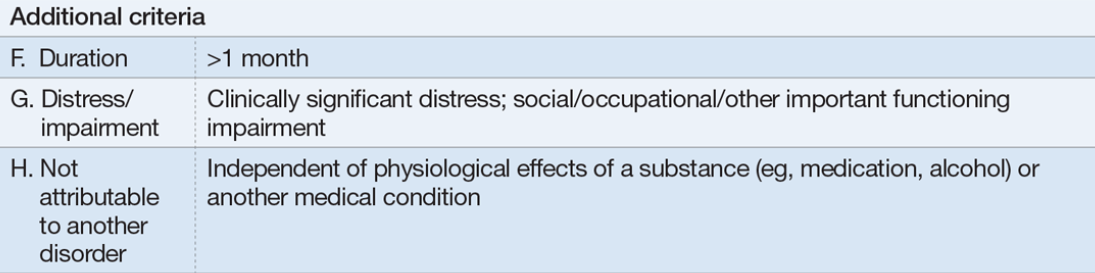
### Posttraumatic stress disorder PTSD
|
||||
|
||||
- Posttraumatic Stress Disorder (cont.)
|
||||
- Trauma and stressor-related disorder
|
||||
- DSM classification
|
||||
- Combat, rape, concentration camp, natural disaster
|
||||
- Examples of Causes
|
||||
- Combat, rape, concentration camp, natural disaster
|
||||
- Clinical description
|
||||
- Trauma memory re-experienced involuntarily, with same emotional force
|
||||
- Symptoms last for at least 1 month
|
||||
|
||||

|
||||
|
||||
|
||||
|
||||
#### Prevalence of PTSD in General Population
|
||||
|
||||
- Lifetime prevalence rate in the U.S. is 6.8%
|
||||
- Higher rates in women despite finding that men are more likely to be exposed to traumatic events
|
||||
|
||||
Research suggests that the higher prevalence of PTSD in women despite men being more likely to be exposed to traumatic events may be due to differences in coping mechanisms, social support, and biological factors.
|
||||
Women may be more likely to seek help and support after a traumatic event, while men may be more likely to suppress their emotions and avoid seeking help.
|
||||
Additionally, hormonal differences between men and women may play a role in how they respond to and recover from traumatic events.
|
||||
|
||||
#### Rates of PTSD After Traumatic Experiences
|
||||
|
||||
- Natural and human disasters
|
||||
- Human intent
|
||||
- Degree of exposure
|
||||
- PTSD definition & assessment
|
||||
|
||||
#### Causal Factors in Posttraumatic Stress Disorder
|
||||
|
||||
##### Individual Risk Factors
|
||||
|
||||
- Lack of college education
|
||||
- Conduct problem
|
||||
- Family history of psychiatric disorder
|
||||
- Scoring high on measures of extraversion and neuroticism
|
||||
|
||||
##### Biological Factors
|
||||
|
||||
- Genetics:
|
||||
5HTTLPR gene
|
||||
- Reduced size of hippocampus:
|
||||
Brain site related to memory & stress response
|
||||
|
||||
##### Sociocultural Factors
|
||||
|
||||
- Higher risk for PTSD
|
||||
- Membership in minority group
|
||||
- Returning to negative and unsupportive social environment
|
||||
|
||||
- In combat-related trauma:
|
||||
- Justification for combat
|
||||
- Identification with combat unit
|
||||
|
||||
## Prevention and Treatment of Stress Disorders
|
||||
|
||||
### Advanced preparation of stressor (Inoculation training)
|
||||
|
||||
- Military service
|
||||
- Medical procedures
|
||||
- Relationship termination
|
||||
|
||||
### Approaches to treatment include:
|
||||
|
||||
- Telephone hotlines
|
||||
- Crisis intervention
|
||||
- Psychological debriefing
|
||||
- Medications
|
||||
- Cognitive-behavioral treatments
|
||||
Reference in New Issue
Block a user